Ketogenic Diets, Ketoacidosis and SGLT-2 Inhibitors - Part 1
Written by: Richard Feinman
Historically — before the discovery of insulin — reduction in dietary carbohydrate or total caloric restriction was the only reliable treatments for diabetes. High blood sugar (hyperglycemia) is the most salient feature of diabetes and the nutritional approach — particularly low-carbohydrate/ketogenic diets — and remains the most effective therapy. However, while even pharmaceutical advertisements recommend drugs “when diet and exercise are not enough,” current medical practice tends to emphasize pharmacology. This, despite the overwhelming successes of carbohydrate restriction in the last few years.[1-4].
The numerous diabetes drugs that are out there have attacked the problem in innovative ways but it is still best understood as a disease of carbohydrate intolerance with high blood sugar being targeted with pharmacology. Many of these drugs are effective but all have side effects and none can really provide the kind of consistent stable glycemic control possible with low-carbohydrate/ketogenic diets.
A relatively new class of drugs, the SGLT-2 (sodium-glucose transporter-2) inhibitors, control blood glucose by preventing re-uptake of glucose that might normally be excreted in the urine. These drugs suffer from a serious side effect — a risk of ketoacidosis, the long-standing threat of (particularly) untreated type 1 diabetes. Ketosis and its relation to ketoacidosis and to ketogenic diets remains a source of some confusion and I will try to provide some background and the role of ketogenic diets.
Pharmacology for diabetes.

Humans have evolved multiple mechanisms to insure that blood glucose is maintained at a relatively constant level. Under normal conditions, to prevent excretion of glucose in the urine, the kidney contains proteins that transport the sugar back into the circulation from the tubules (Figure 1). The sodium-glucose transport proteins (SGLTs) and, in particular, the SGLT-2 forms, provide the mechanism for the re-uptake of glucose that has been filtered. In diabetes, the system may not be able to keep up with the high blood glucose.
SGLT-2 is a so-called synport or co-transporter, meaning that it carries glucose and sodium together back into the circulation. The energy to drive the transport comes from a sodium gradient created by an an ATP-dependent Na-K exchanger. The idea is that if one can find an inhibitor of the SGLT-2 protein, one can use this system as a strategy for treating diabetes. Several SGLT-2 inhibitors have been developed. This class of drugs blocks the re-uptake allowing glucose to be excreted in the urine [5-7]. The reduction in glucose and the associated reduction in insulin may lead to ketosis (as described below) but, for unknown reasons, this may become excessive. Because the ketone bodies are acids, one of the serious side-effects of SGLT-2 inhibitors is ketoacidosis, the life-threatening effect of unregulated ketosis; an FDA warning was issued in 2015 and recently updated [7]. The punch-line is that ketogenic diets rarely lead to ketoacidosis and, in fact, reduce the need for SGLT-2 inhibitors in patients taking these drugs.
Regulation of Ketosis.
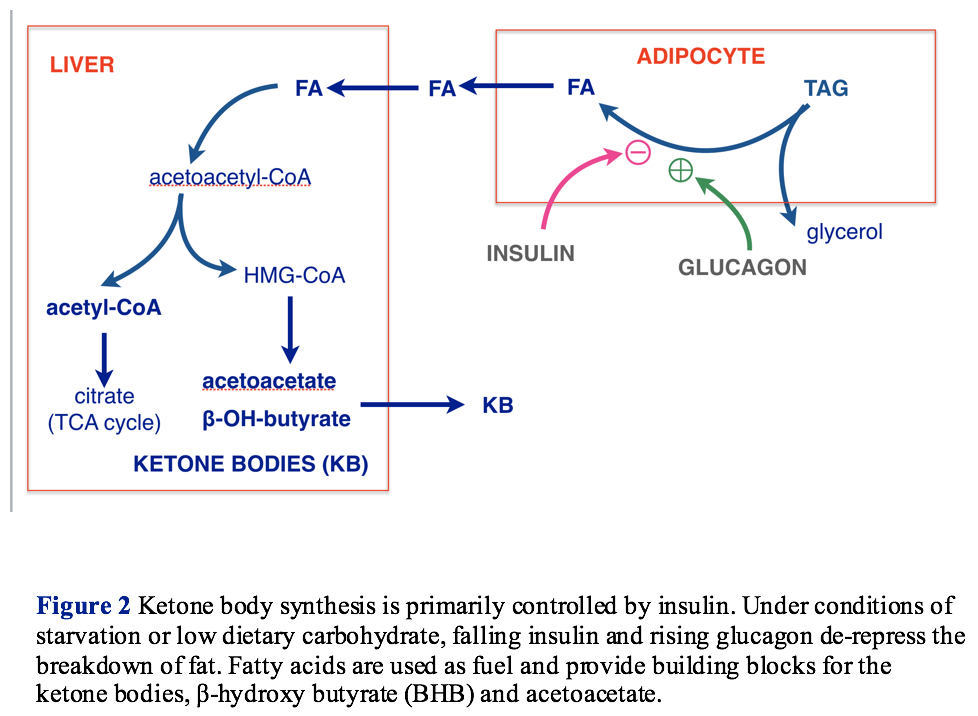
Under conditions of starvation or low carbohydrate intake, the reduction in insulin (and increase in glucagon) that follows from low glucose leads to breakdown of fat (lipolysis) to fatty acids. Fatty acids then become the major fuel providing acetyl-CoA (the two-carbon fragment that is the essential fuel for oxidative metabolism). Low insulin, in combination with other metabolites, stimulates ketogenesis, the assembly of acetyl-CoA units into the four-carbon ketone bodies, β-hydroxy butyrate (BHB) and acetoacetate (Figure 2).
Ketone bodies, made in the liver, are exported to other cells, particularly muscle and brain where they can be turned back into acetyl-CoA and used for energy. Big generalization: the role of ketone bodies is to transport acetyl-CoA from the liver to the periphery.

Under normal conditions, the ketone bodies regulate their own synthesis. Ketone bodies can feed back to adipose tissue and repress lipolysis, thereby reducing the supply of fatty acids for synthesis. In addition, ketone bodies stimulate the pancreas to release insulin. (Figure 3)
So, normally, there is a long feedback loop: low glucose ➛ low insulin ➛ increase lipolysis ➛ fatty acids ➛ ketone bodies ➛ increase insulin ➛inhibit lipolysis ➛ decrease fatty acids ➛ decrease ketone bodies ➛ low insulin ➛ increase lipolysis, and so on. This is the control system that keeps ketogenic diets from running out of control and prevents acidosis in normal people (Figure 3). This is the system that goes wrong in type 1 diabetes.

Type 1 Diabetes and the Threat of Ketoacidosis.
With no insulin and, thereby, loss of the ability to turn off fatty acid production, the type 1 patient is at risk for unregulated ketone body production, that is, ketoacidosis (Figure 4). Historically, this was the major threat in diabetes. Because ketoacidosis in the clinic appears in untreated or inadequately controlled type 1, where there is a generally also high blood glucose, there is the expectation that ketoacidosis and hyperglycemia will appear together. The medical literature indicates that, in the case of SGLT-2 where the glucose becomes controlled, acidosis can be missed, and reference is made to “euglycemic ketoacidosis,” but the mechanisms in type 1 and the side effect of SGLT-2 inhibitors are likely the same. It is not the high glucose but, rather, the very low or absent insulin, that is the source of the problem in type 1. (Ketosis is the response to low insulin, and normally, high glucose in a normal person would repress ketosis).
Treating diabetes with insulin will allow reinstatement of the controlling feedback loop, but administering external insulin cannot really provide the continuous smooth regulation that keeps blood glucose constant [10]. There remains the possibly of continued fluctuations in blood glucose (and therefore insulin) and that can lead to ketoacidosis. Part 2 will discuss what goes wrong in treatment with SGLT-2 Inhibitors.
References
1. Hallberg, S.J., McKenzie, A.L., Williams, P.T. et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Ther 9, 583–612 (2018) doi:10.1007/s13300-018-0373-9
2. Athinarayanan SJ, Adams RN, Hallberg SJ, et al. (2019) Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes: A 2-Year Non-randomized Clinical Trial. Front. Endocrinol. 10:348. doi: 10.3389/fendo.2019.00348
3. Hallberg SJ, Dockter NE, Kushner JA, Athinarayanan SJ. Improving the scientific rigour of nutritional recommendations for adults with type 2 diabetes: A comprehensive review of the American Diabetes Association guideline-recommended eating patterns. Diabetes Obes Metab. 2019;21:1769–1779. https://doi.org/10.1111/ dom.13736
4. Lennerz,BS, Barton A, Bernstein RK, et al. Management of Type 1 Diabetes With a Very Low–Carbohydrate Diet. Pediatrics. 2018;141(6):e20173349,
5. Joffe, D. (2018 ) SGLT2 Inhibitors: A New Class of Diabetes Medications. Diabetes In Control, Sep.19, 2018 http://www.diabetesincontrol.com/sglt2-inhibitors-a-new-class-of-diabetes-medications/
6. Rosenstock, Ferrannini, E. (2015) Euglycemic Diabetic Ketoacidosis: A Predictable, Detectable, and Preventable Safety Concern With SGLT2 Inhibitors. Diabetes Care; 38:1638–1642 |. DOI: 10.2337/dc15-1380
7. Food and Drug Administration. (2015) FDA Drug Safety Communication: FDA warns that SGLT2 inhibitors for diabetes may result in a serious condition of too much acid in the blood. http://www.fda.gov/Drugs/DrugSafety/ucm446845.htm. Accessed May 25, 2015.
8. Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition 2015;31:1–13
9. FARXIGA (datagliflozin) website https://www.farxiga-hcp.com/t2d-hospitalization-heartfailure.html last accessed February 4, 2020.
10. Derr, et al. (2003 ) Is HbA1c Affected by Glycemic Instability? Diabetes Care 26(10): 2728-2733. https://doi.org/10.2337/diacare.26.10.2728
11. American Diabetes Association. Chapter 4. Lifestyle management: Standards of Medical Care in Diabetes 2018. Diabetes Care 2018;41(Suppl. 1):S38–S50
12. American Diabetes Association. Standards of medical care in diabetes. Chapter 5: lifestyle management. Diabetes Care. 2019;42:S46-S60.
13. Kosiborod M, Lam CSP, Kohsaka S, et al. Cardiovascular Events Associated With SGLT-2 Inhibitors Versus Other Glucose-Lowering Drugs: The CVD-REAL 2 Study. J Am Coll Cardiol. 2018 71(23):2628-2639. doi: 10.1016/j.jacc.2018.03.009.